

Authors: Muhammad Hamza, Aziz Ur Rehman, Usman Ali, Faisal Rehman
Affiliation: University of Veterinary and Animal Sciences Lahore, Sub Campus Jhang
Various species of Ebola virus, notorious for causing highly lethal hemorrhagic fever with mortality rates ranging from 90pc to 95pc and designated as a biosafety level 4 agent, especially the Zaire Ebola virus, have been associated with human outbreaks since its first appearance in 1976 near the Ebola River in South Sudan and the Democratic Republic of the Congo.
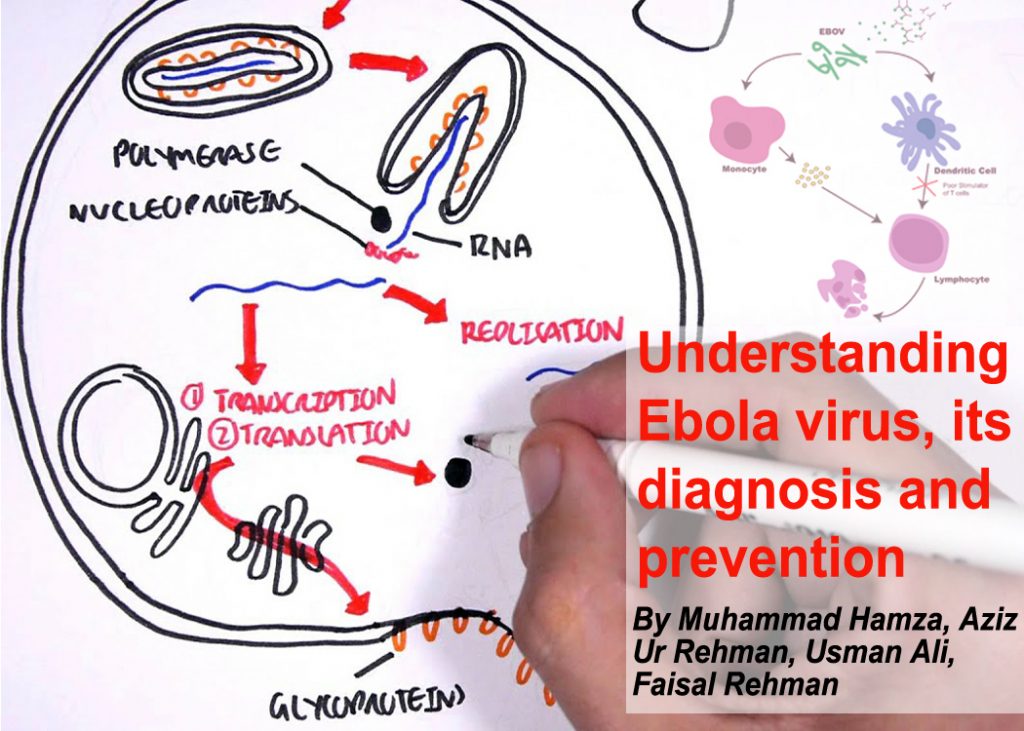
A member of the Filoviridae family, Ebola virus represents a formidable threat due to its negative-sense ssRNA structure, enveloped pleomorphic nature, and replication in the cytoplasm.
Natural hosts of the Ebola virus are bats of the Pteropodidae family. Human transmission occurs through close contact with infected animals, including fruit bats, chimpanzees, gorillas, and monkeys.
Transmission primarily happens via blood, secretions, organs, or bodily fluids. Human-to-human transmission can also occur through direct contact with infected individuals, contaminated objects, and during burial ceremonies. Importantly, transmission only occurs when an infected person displays signs and symptoms, with an incubation period ranging from 2 to 21 days.
The 19kb long Ebola virus genome encodes various structural and nonstructural proteins crucial for virus attachment, replication, and immune evasion. Notable proteins include the virion envelope glycoprotein (GP), nucleoprotein (NP), matrix proteins VP24 and VP40, nonstructural proteins VP30 and VP35, and the viral polymerase.
Ebola virus enters the human body through mucous membranes and skin breaks, infecting various cell types. The surface glycoprotein GP facilitates infection, leading to the virus spreading to lymph nodes, liver, spleen, and adrenal glands. This process results in lymphocyte apoptosis, hepatocellular necrosis, clotting dysregulation, and multiorgan failure.
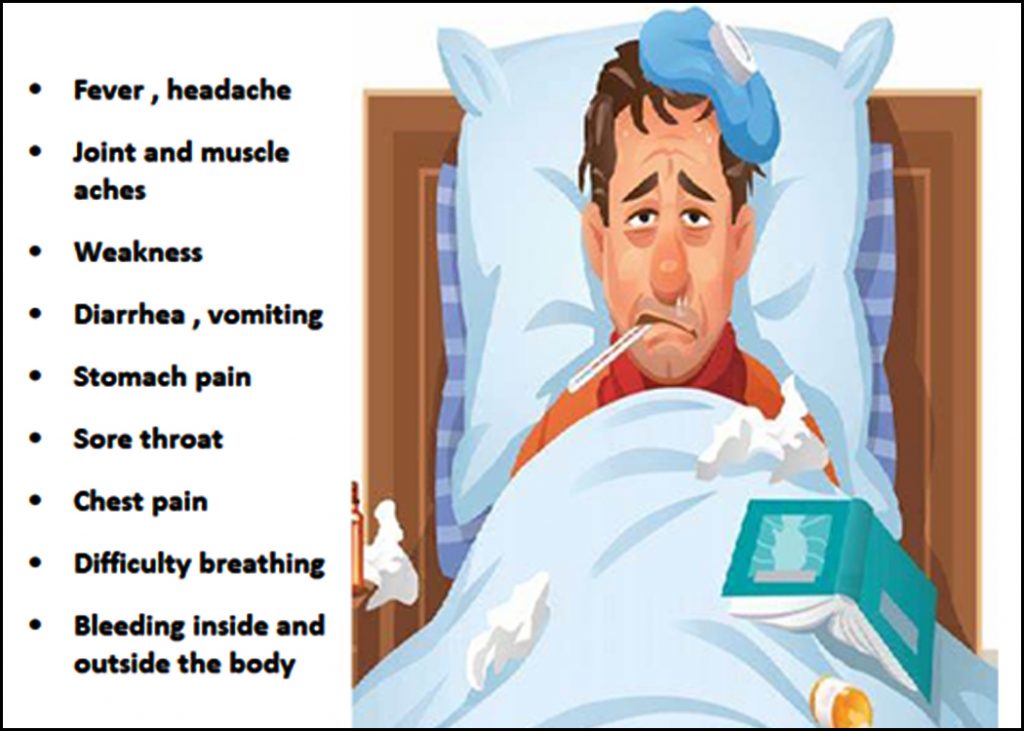
Symptoms of Ebola virus infection include fever, myalgia, chills, and malaise, often resembling those of other hemorrhagic fevers.
Handling the Ebola virus requires biosafety level 4 laboratories. Rapid diagnosis is facilitated by mobile diagnostic labs deployed in outbreak settings. Disinfection methods include Lysol, microchem plus, and hypochlorite solutions. Tests such as CBC, ELISA, immunofluorescent assays, RT-PCR, and rapid diagnostic tests are employed for diagnosis.
Preventive measures include proper hand washing, avoiding contact with the body fluids of infected individuals, vaccination, reducing wildlife-to-human transmission, safe burial practices, minimising sexual transmission risk, and handling pregnancy-related fluids and tissues with care.
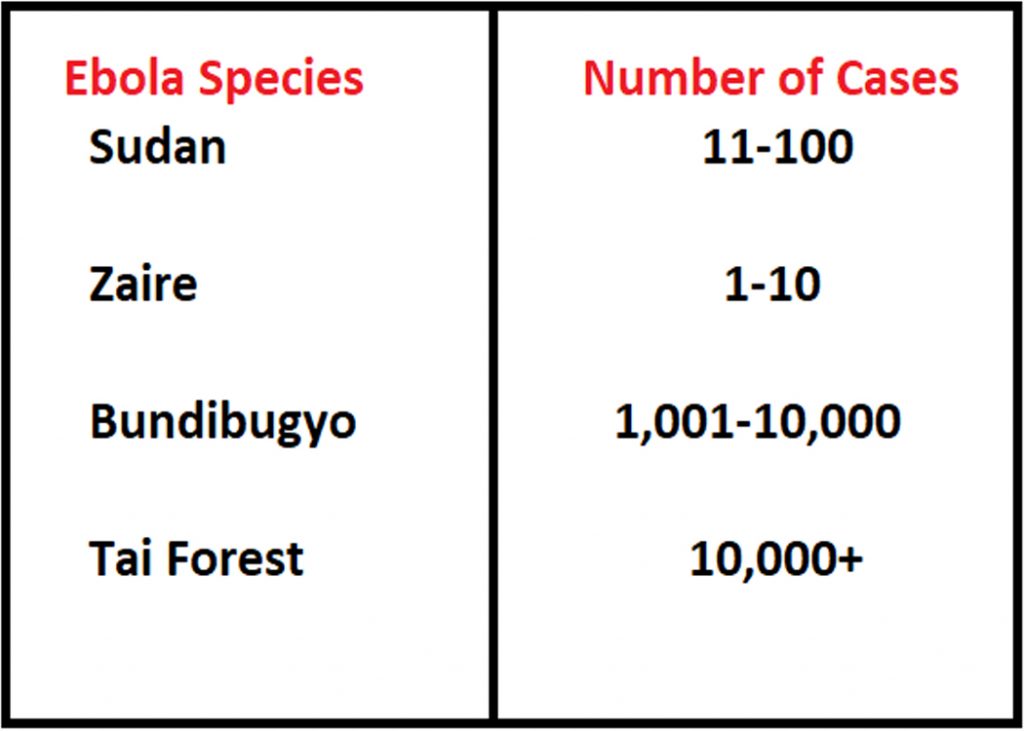
Ebola is not prevalent in Pakistan and is not recognised as an epidemic. The average case fatality rate is around 50pc, with rates varying in past outbreaks.
Rapid and efficient diagnosis is crucial for containing Ebola outbreaks and preventing them from escalating into health emergencies. Swift diagnosis significantly impacts the spread of infection, reducing the attack rate and ultimately saving lives.


